Program Signaling in the Residency Match: How Gold and Silver Signals Actually Work
May 18, 2026
IMGPrep · Strategic Guide · 2026
What Program Signaling Is
A program signal is a standardized, private indicator of interest attached to an ERAS application. Each participating specialty grants applicants a fixed number of signals. The applicant selects which programs receive them. Programs that receive a signal see it; programs that did not are not told you chose to signal elsewhere. There is no leaderboard.
Program signaling residency strategy solves a specific problem. By the late 2010s, residency programs in competitive specialties were receiving more than a thousand applications per cycle for a handful of positions. Programs could not distinguish genuine interest from algorithmic mass-applying, and applicants could not distinguish programs that would seriously read their materials from programs that would screen them out unread. Both sides were operating without information.
Signaling restores information to the system. By making signals scarce, the mechanism forces applicants to reveal which programs they actually care about. Programs can then prioritize reading those applications. The signal is credible precisely because it is costly: every signal spent on one program is a signal not spent elsewhere.
A Brief History of Program Signaling Residency Implementation
Preference signaling did not originate in medicine. It originated in economics. In 2006, the American Economic Association launched a signaling mechanism for the new-PhD job market, allowing each candidate to send a small number of private signals of interest to employers ahead of interview decisions. The mechanism was formalized in a 2010 NBER working paper by Peter Coles, Alexey Kushnir, and Muriel Niederle, which became the conceptual blueprint for signaling in two-sided matching markets — markets where one side cannot give full attention to every applicant on the other side.
In the 2020–2021 application cycle (the 2021 Match), Otolaryngology–Head and Neck Surgery became the first medical specialty to pilot preference signaling. Each applicant received five signals. Every otolaryngology residency program participated. The differential was unambiguous: signaled programs offered interviews at roughly 48 to 58 percent, versus 10 to 14 percent for unsignaled programs — a four- to five-fold effect (Pletcher 2022, Academic Medicine). Applicants and program directors both endorsed continuation.
The model spread quickly. 2021: Otolaryngology pilots with 5 signals. 2022: Urology adopts signaling independently; ERAS introduces signaling for General Surgery, Dermatology, and Internal Medicine. 2023: ERAS expands to 15 specialties; 17 total specialties now use signaling, covering more than 80 percent of residency applicants. 2024 onward: Family Medicine, Pediatrics, and additional specialties join. Tiered Gold/Silver structures are introduced in Internal Medicine, Anesthesiology, Dermatology, Diagnostic Radiology, Obstetrics-Gynecology, and several IM-based fellowships. For the 2026 MyERAS cycle, at least 27 specialties accept signals.
Three Features That Define How Signals Work
Signals are capped. You cannot signal every program. The cap is the engine of the mechanism: scarcity is what makes the signal credible. A signal you could give to anyone would communicate nothing.
Signals are private. A program sees that you signaled it. It does not see which other programs you signaled, which you did not, or which you intend to rank higher. Signaling is informational, not competitive.
Signals are pre-interview, not pre-rank. Program signaling residency mechanisms operate at the point where programs decide whom to interview. They are explicitly not ranking tools. The Alliance for Academic Internal Medicine, which governs Internal Medicine signaling, states this directly: programs should not use signals for rank-list decision-making. Most participating specialties echo that guidance. The downstream evidence supports it — programs do not significantly rank signaled applicants higher than non-signaled ones on final rank order lists.
Gold and Silver — The Two-Tier Signaling System
A growing list of specialties has adopted a two-tier signaling system that distinguishes two intensities of interest. Single-tier specialties give every signal the same weight. Tiered specialties give applicants a small number of high-weight Gold signals and a larger pool of standard-weight Silver signals.
Gold Signal
“Most preferred”
The highest level of expressed interest. Typically three to six per specialty.
Published effect (IR): 54% interview rate, odds ratio 9.66.
Silver Signal
“Preferred”
Strong interest, but explicitly below Gold. Typically ten to twenty-five per specialty.
Published effect (IR): 40% interview rate, odds ratio 4.69.
The comparison data is the clearest in the published literature. In Obstetrics-Gynecology, Gold signals yielded a 64 percent interview rate; Silver signals yielded 44 percent; unsignaled applications received interviews at roughly 6 to 10 percent. Both Gold and Silver dramatically outperform no signal at all. Gold roughly doubles the effect of Silver.
Two practical observations follow from the data. First, Silver signals are not consolation prizes. They are powerful interview-acquisition tools in their own right — a Silver signal in Interventional Radiology nearly quintupled the odds of an interview. Applicants who under-spend their Silver allocation surrender most of the mechanism’s benefit. Second, Gold signals are not uniformly interpreted across programs. In tiered specialties, roughly two-thirds of program directors weight Gold more heavily than Silver. About one-third report no functional differentiation — for those programs, what matters is that a signal was sent at all.
Which Specialties Use Program Signaling in 2026
At least 27 specialties participate in program signaling for the 2026 application season. Most run through ERAS, but two specialties — Obstetrics & Gynecology and Emergency Medicine — have moved off ERAS entirely and deliver signals through ResidencyCAS. The mechanism is the same; the platform is different. Signal allocations are reset by specialty, so candidates applying across specialties do not share a pool.
| Specialty | Structure | Total | Platform |
|---|---|---|---|
| Tiered (Gold & Silver) | |||
| Anesthesiology | 5G / 10S | 15 | ERAS |
| Dermatology | 3G / 25S | 28 | ERAS |
| Diagnostic Radiology | 6G / 9S | 15 | ERAS |
| Internal Medicine | 3G / 12S | 15 | ERAS |
| Obstetrics & Gynecology | 3G / 15S | 18 | ResidencyCAS |
| Single-Tier (Equal Weight) | |||
| Emergency Medicine | Equal | 5 | ResidencyCAS |
| Family Medicine | Equal | 5 | ERAS |
| General Surgery | Equal | 15 | ERAS |
| Neurology | Equal | 8 | ERAS |
| Neurological Surgery | Equal | 25 | ERAS |
| Orthopedic Surgery | Equal | 30 | ERAS |
| Otolaryngology | Equal | 25 | ERAS |
| Pediatrics | Equal | 5 | ERAS |
| Psychiatry | Equal | 10 | ERAS |
| Urology | Equal | 30 | ERAS |
Sources: AAMC, Program Signaling for the 2026 MyERAS Application Season (ERAS specialties); ACOG/APGO and CORD guidance (ResidencyCAS specialties). Table is illustrative; additional specialties and IM-based fellowships also participate.
ResidencyCAS Signaling: Obstetrics & Gynecology and Emergency Medicine
Two specialties have moved off ERAS entirely and now deliver program signaling residency mechanics through ResidencyCAS, a platform built by Liaison and adopted by ACOG (2024–2025 cycle) and CORD (2025–2026 cycle). The signaling concept is identical — scarce, private, pre-interview indicators of interest — but applicants in these two specialties register, apply, signal, and interview entirely outside the ERAS ecosystem. IMG applicants should plan their application logistics accordingly: ECFMG authorization works differently for ResidencyCAS, and the document workflow does not mirror MyERAS.
Obstetrics & Gynecology · ResidencyCAS
18 signals — 3 Gold + 15 Silver
OB-GYN transitioned to ResidencyCAS for the 2024–2025 cycle. The platform was developed by ACOG with the Right Resident, Right Program, Ready Day One initiative to support holistic review and the Alignment Check Index. Applicants register through ResidencyCAS, not MyERAS — and for IMGs, that registration runs through ECFMG’s OB-GYN-specific support workflow.
Emergency Medicine · ResidencyCAS
5 signals — single-tier
EM transitioned to ResidencyCAS for the 2025–2026 cycle following the 2022–2023 cycles in which more than 550 positions went unfilled despite an adequate applicant pool. CORD’s explicit guidance: do not signal core EM home or away rotation sites — those programs already have direct information about you. Reserve signals for high-fit programs without a pre-existing relationship.
For Emergency Medicine applicants, signaling sits alongside the Standardized Letter of Evaluation (SLOE) — the specialty’s dominant selection instrument. The SLOE is what gets your application read; the signal directs that read toward the programs you are most aligned with. For IMG applicants without access to U.S. EM rotations, this combination is what determines whether a competitive application reaches the interview stage. See the EM IMG Strategic Guide for the full selection architecture.
For OB-GYN applicants, the Gold/Silver distinction matters more than in most specialties because the Alignment Check Index (ACI) tool encourages applicants to signal programs where structural fit is genuine rather than aspirational. A Gold signal sent to a program with no documented IMG match history burns one of only three Gold tokens you have. For the OB-GYN application timeline, registration workflow, and signal mechanics, see the OB-GYN ResidencyCAS guide.
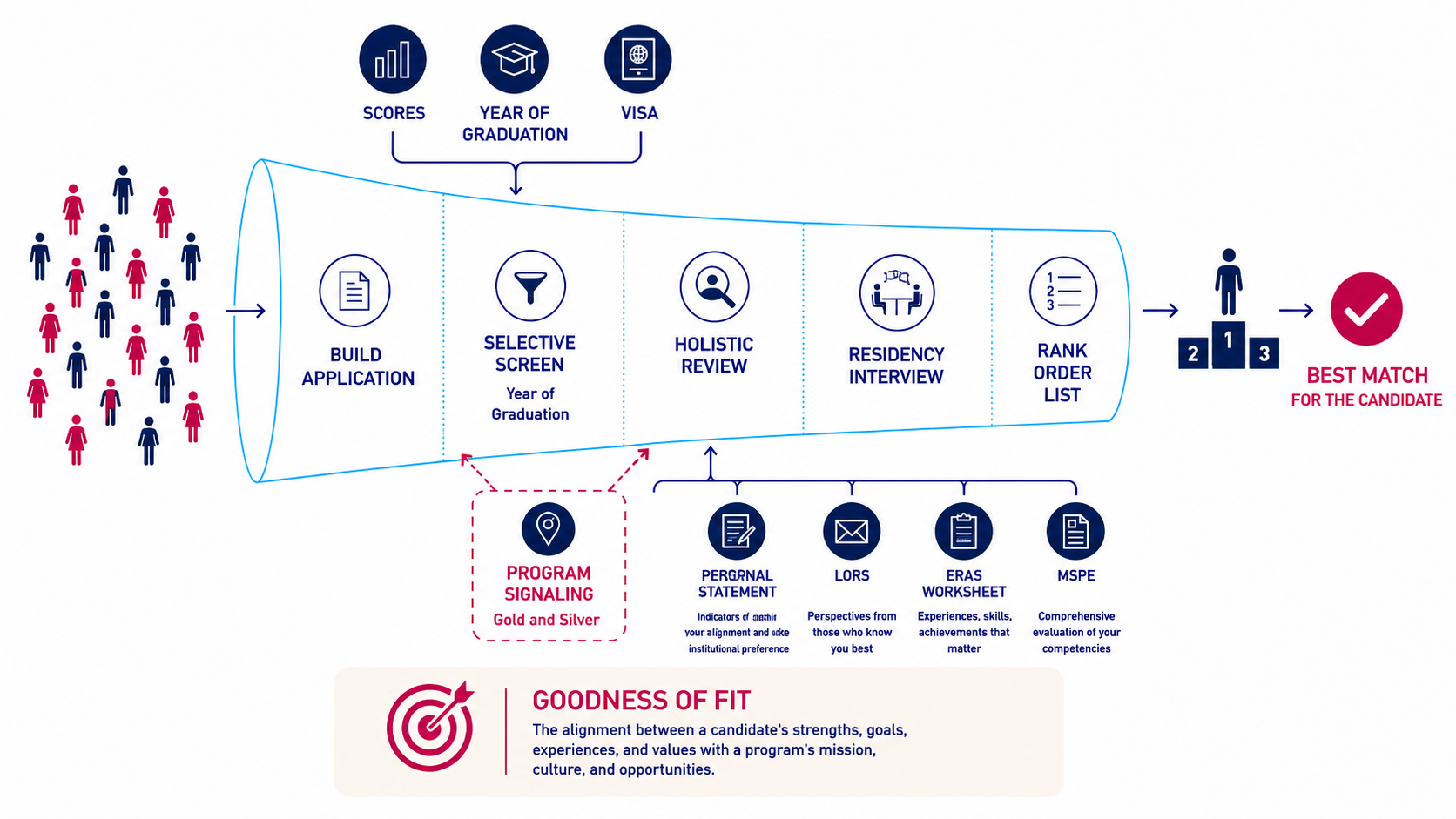
Where Program Signaling Sits in the Match Funnel
Program signaling residency strategy is most useful when understood as a specific stage of the selection process — not as a general advantage that lifts every application. IMGPrep frames this stage within the broader screening-to-holistic-review architecture that governs all residency selection.
The Match Funnel proceeds in four selection phases. Programs first apply binary filters — ECFMG certification, year of graduation, visa sponsorship capability, USMLE pass status. Applicants who fail any binary filter are removed entirely. Programs then apply quantitative filters — Step 2 CK score thresholds, U.S. Clinical Experience hours, research output. Applicants who clear both filter layers enter holistic review, where committees read personal statements, letters of recommendation, the MSPE, and the ERAS worksheet. Holistic review feeds interview selection and ultimately the rank order list.
Signaling operates at the transition from selective screening into holistic review. The stage-by-stage data is clear.
Application → Interview Invitation. This is where signals have their greatest impact. Across specialties, signaling increases the odds of an interview invitation by roughly five to seven times. In Pediatrics, signaled applicants had 7.15-fold higher odds of an interview invitation. In General Surgery, signaling increased the odds of inclusion on a program’s rank order list by 5.63 times.
Interview Invitation → Interview Completion. Signals continue to matter. Pediatrics data showed that applicants who signaled had 4.82-fold higher odds of completing an interview once invited.
Interview → Rank List Inclusion. The signal’s direct effect diminishes here. Most programs do not consult signals when constructing rank lists. However, the correlation between signaling and genuine interest produces an indirect effect: signaled applicants are more likely to themselves rank the program highly, creating mutual alignment.
Match Outcome. The downstream data is striking. In Orthopedic Surgery, 90 percent of matched applicants matched at a program they had signaled. In Urology, 95 percent of matched applicants matched at a signaled program. In Obstetrics-Gynecology, 71 percent matched at a Gold- or Silver-signaled program.
Two implications follow from where signals sit in the funnel. First, signaling does not move applicants past the binary filters. If a program does not sponsor J-1 visas, a Gold signal does not change that. If a program filters on year-of-graduation thresholds, a Gold signal does not adjust the threshold. Second, signaling does not appear on the rank order list. Once the interview is given, the signal has done its work; rank position is determined by interview performance, fit, and the program’s independent assessment.
For IMG Applicants · Funnel Note
For IMGs, the funnel has an additional structural layer before signaling enters the picture.
U.S. MD and DO seniors typically clear the binary filter layer automatically. For IMGs, binary filters are the most consequential stage of the entire Match. The 2026 NRMP Match data confirmed this empirically: permanent residents matched at 67.9 percent, while applicants requiring visa sponsorship matched at 54.4 percent — a 13.5-point gap, validating visa status as a first-order structural filter.
The implication for program signaling residency strategy is direct: a signal of any tier sent to a program that does not accept your visa type, your year of graduation, or your U.S. Clinical Experience profile is structurally invisible. The program will not see the signal until it has already screened you out. IMG signal strategy is therefore an exercise in confirming structural eligibility before spending any signal — Gold or Silver.
How Programs Actually Use Signals
Survey data from program directors shows a clear pattern of how signals are used at each step:
81%
Initial Screening
of program directors use signals when deciding which applications to read carefully.
62%
Interview Offers
use signals when deciding which applicants to invite for interviews.
9%
Rank List
use signals when constructing the rank order list. Signals are an interview-acquisition tool, not a ranking tool.
The asymmetry is the most important pattern in the entire literature. Signals are a screening and invitation mechanism. They get your application read, and they help convert that reading into an interview. They do not function as a ranking lever after you have been interviewed. Once you are in the interview room, performance, fit, and the impression you make determine rank position — not the signal.
There is also strong evidence that signals identify candidates who would otherwise have been overlooked. In one analysis, 71 percent of program directors agreed that signals helped them identify strong applicants they might not have flagged from a raw application pool. This is the equity case for program signaling residency strategy, and it is real: signals can pull genuinely competitive applicants past the noise floor.
The Diminishing Returns Problem
A cross-specialty analysis of the ten most competitive specialties produced one of the most counterintuitive findings in the signaling literature: as the number of available signals increases, the value of each individual signal decreases.
Cross-Specialty Finding
In specialties offering 10 signals or fewer, each signal carried an odds ratio of 5.99 for matching at a signaled program.
In specialties offering 20 signals or more, that odds ratio dropped to 3.00 — roughly half the per-signal power.
Scarcity is what makes a signal credible. When a specialty offers thirty signals, a program receiving one of them learns relatively little about the applicant’s commitment. When a specialty offers three Gold signals, a program receiving one learns a great deal.
For applicants in low-signal specialties (Family Medicine, Pediatrics, Otolaryngology with 5 signals each), every allocation decision carries significant weight. For applicants in high-signal specialties (Orthopedic Surgery, Urology with 30 signals each), the strategic emphasis shifts: signals function less as differentiators and more as table-stakes; programs in those specialties may interview only applicants who signaled them.
The Away Rotation Caveat — What Signals Cannot Replace
One of the most important findings from the cross-specialty literature is rarely discussed in signaling guides. In an analysis of the ten most competitive specialties, the strongest predictor of matching at a given program was not signaling. It was completing an away rotation at that program.
OR 9.25
Away Rotation
Strongest single predictor of matching at a specific program.
OR 7.74
Gold Signal
Powerful, but second to an established in-person relationship.
This finding has direct strategic consequences. If you completed an away rotation at a program, that program already has more information about you than any signal can convey. Spending a scarce Gold signal there is likely informationally redundant. The smarter move is to use Silver at the away program (or signal another program where the program has no other reason to know you) and reserve Gold signals for high-fit programs with no pre-existing relationship.
For IMG applicants, the away rotation equivalent is a hands-on U.S. Clinical Experience rotation at a program with an active residency in your target specialty. Most signaling guidance recommends signaling the away program in some form as a safe default — but using Silver rather than Gold, and freeing the Gold signal for a target where it carries marginal information.
A Strategic Framework for Allocating Signals
Program signaling residency allocation should follow three sequential checks. The order matters: a signal fails if any earlier check is missed, regardless of the later checks.
Check 1
Structural eligibility
Does the program accept your visa type, year of graduation, and USMLE profile? If any binary filter fails, the signal is wasted. Verify before allocating.
Check 2
Quantitative threshold
Does your Step 2 CK, research output, and USCE profile clear the program’s quantitative screen? Signals do not move the screen; they only matter once you have cleared it.
Check 3
Narrative fit
Can you articulate, in the personal statement and during interviews, why this program in particular? Signals expressing genuine fit outperform signals expressing prestige preference.
Beyond the three checks, several allocation principles emerge consistently from the published literature.
Allocate Gold across your competitiveness band, not only at the top. A radiology applicant survey, one of the few published studies of allocation strategy, found that applicants matched at higher rates when they spread Gold signals across likely-to-match, aspirational, and safety programs — roughly three Gold to likely-match, two Gold to aspirational, and one to a safety. Stacking every Gold signal at the top of the perceived prestige curve dilutes their effect.
Use Silver as deliberately as Gold. Silver signals are not residual allocations. A Silver signal in Interventional Radiology produced an OR of 4.69 for an interview — nearly five times the unsignaled baseline. Silver signals are powerful interview-acquisition tools in their own right. Applicants who treat them as filler underperform.
Do not spend Gold where you already have a relationship. Away rotations, home programs, and programs that have hosted you carry their own information advantage. An away rotation is a stronger predictor of matching than any signal. Use Silver at these programs (or skip the signal entirely if program policy advises) and reserve Gold for high-fit programs with no pre-existing connection.
Geographic alignment compounds signal value. Most specialties now pair program signals with geographic preferences. A signal sent within a geographic region you explicitly preferred carries more weight than the same signal sent in isolation — published data show that combining a preference signal with a geographic preference roughly tripled the odds of an interview and increased the odds of matching more than sixfold compared with using neither.
Use every available signal. Across every specialty studied, applicants who used their full signal allocation matched at higher rates than those who held signals in reserve. There is no strategic value to unspent signals.
For IMG Applicants · Signal Allocation
For IMGs, the three-check framework requires an additional layer: the SUVY filters.
U.S. MD seniors signaling Internal Medicine programs can usually assume binary clearance. IMGs cannot. The SUVY framework — Scores, U.S. Clinical Experience, Visa, Year of Graduation — defines whether a program will read your application at all. A signal of any tier sent to a program that filters out applicants with J-1 sponsorship requirements, with a graduation year beyond a four- or five-year window, or without specific USCE thresholds is structurally invisible.
The 2026 NRMP data made the visa filter measurable. Non-U.S. IMGs needing visa sponsorship matched at 54.4 percent, a five-year low. Permanent residents matched at 67.9 percent. The 13.5-point gap is the structural cost of misallocating signals to programs that do not sponsor your visa type. This applies to both Gold and Silver signals: tier does not override a binary filter.
Before allocating any signal as an IMG, confirm three things about each candidate program: that it has interviewed applicants with your visa type within the last three cycles, that it has accepted applicants within your year-of-graduation window, and that its IMG match rate is not zero. A Customized Residency Program List performs this filtering at scale; the same discipline can be done manually using NRMP and program-published data, with substantially more time.
What Program Signaling Cannot Do
Program signaling residency mechanisms have been promoted aggressively by application advisory services, sometimes in language that overstates their effect. A clear-eyed account of the limits is more useful than the marketing version.
Signaling cannot override binary filters. If a program does not sponsor your visa type, a Gold signal does not change that. If a program will not consider applicants more than three years out from graduation, a Gold signal does not shift the threshold. Binary filters precede signaling in the funnel.
Signaling cannot substitute for application quality. A weak personal statement, thin letters, an MSPE without strong narrative threads — none of these are fixed by a signal. Signaling moves you into holistic review; what holistic review finds is what your application contains.
Signaling cannot replace an away rotation. The published cross-specialty data is unambiguous: an away rotation is a stronger predictor of matching at a specific program than any signal, including Gold.
Signaling does not function as a rank-order indicator. Specialty governance bodies have stated this explicitly, and the published data support it. Once an applicant interviews, signals are not consulted again. Rank position is determined by interview performance and fit.
Signaling does not guarantee an interview. The signal raises probability; it does not deliver an outcome. Even at programs where signaling is decisive, applicants are evaluated against the rest of the pool.
Goodness of Fit — The Underlying Logic
The Match is best understood as a sorting mechanism producing fit between applicants and programs. It is not a lottery, and it is not a pure competition. Programs are looking for residents who will thrive in their specific environment; applicants are looking for programs aligned with their goals, geographies, and career trajectories.
A signal — Gold or Silver — is a tool for densifying the funnel where structural fit and applicant preference converge. It is most valuable when it points to a program where the applicant is structurally eligible, quantitatively competitive, narratively aligned, and genuinely interested. In that intersection, the signal accelerates the program’s identification of a strong-fit applicant. Outside that intersection, it accomplishes nothing.
Applicants who treat program signaling residency strategy as a scarce strategic resource — allocated by structural eligibility first, then by realistic competitiveness, then by fit, with Gold reserved for cases where the marginal information matters — consistently outperform in the published outcomes data. This is the Goodness of Fit thesis applied to signaling: the signal is most powerful where the underlying alignment already exists, and most wasted where it does not.
Goodness of Fit
The alignment between an applicant’s strengths, goals, experiences, and values and a program’s mission, culture, and opportunities. Signals accelerate program recognition of this alignment when it already exists; they cannot create alignment where the underlying fit is absent.
Related Reading on imgprep.com
- → IMG Friendly Programs and the SUVY Framework
- → Standardized Screening vs Holistic Review in Residency Selection
- → Understanding the NRMP Program Director Survey
- → OB-GYN ResidencyCAS: Step-by-Step Guide
- → Why Emergency Medicine Moved from ERAS to ResidencyCAS
- → Emergency Medicine Residency for IMGs: A Strategic Guide
- → The Emergency Medicine SLOE: A Guide to the Standardized Letter of Evaluation
- → Anesthesiology Residency for IMGs: A Strategic Guide
- → General Surgery Residency for IMGs: A Strategic Guide
- → Strategic Guide for Internal Medicine IMGs
- → How IMGs Match Into Psychiatry Residency
- → Urology Match for IMGs
- → IMG Friendly Residency Programs (2026 Data)
- → Five-Year Analysis: IMG Residency Match Statistics, 2022–2026
- → 2026 U.S. IMG vs Non-U.S. IMG Residency Match Guide
- → What Is the MSPE? A Strategic Guide for IMGs
- → ERAS for IMGs: Complete 2026–2027 Residency Application Guide
- → USMLE Changes 2026: Step 1, Step 2 CK, and Step 3 Update
- → U.S. Clinical Experience (USCE) — Hands-on Externship for IMGs
- → Residency Personal Statement: Writing Tips and Red Flags
- → Customized Residency Program Lists for IMGs
- → Browse All IMGPrep Articles
Sources
- National Resident Matching Program (NRMP). Advance Data Tables: 2026 Main Residency Match. March 2026. Available at nrmp.org.
- National Resident Matching Program (NRMP). Charting Outcomes: Program Director Survey Results, 2024 Main Residency Match. August 2024.
- National Resident Matching Program (NRMP). NRMP Releases Results of the 2026 Main Residency Match. Press release, March 20, 2026.
- Association of American Medical Colleges (AAMC). Program Signaling for the 2026 MyERAS Application Season. Available at students-residents.aamc.org.
- Pletcher SD, Chang CWD, Thorne MC, Malekzadeh S. The Otolaryngology Residency Program Preference Signaling Experience. Academic Medicine. 2022;97(5):664–668. PMID 35234686.
- Grauer R, Ranti D, Greene K, et al. Characterization of Applicant Preference Signals in Urology. JAMA Network Open. 2023;6(1):e2250974.
- Cai F, Southworth E, Santiago S, et al. The Golden Tickets: Impact of Preference Signaling on Obstetrics and Gynecology Residency Applicants. American Journal of Obstetrics and Gynecology. 2024;230(2):262.e1–262.e9.
- Tobin MJ, Raquepo TM, Puducheri S, et al. The Power of a Signal: The Impact of Preference Signaling on Matching in the Top 10 Most Competitive Specialties. Academic Medicine. 2026;101(5):526–534.
- Kim C, Nguyen AT, Anavim S, et al. From Application to Match: Evaluating the Impact of Tiered Signals in Interventional Radiology. Academic Radiology. 2026;33(4):1223–1228.
- Hart R, Ponitz K, Ihsan F, Ben-Zion S. Impact of Preference and Geographic Signaling on Interview and Match Outcomes Among Midwestern Pediatric Residency Applicants. Academic Pediatrics. 2026;26(3):103203.
- Coles PA, Kushnir AI, Niederle M. Preference Signaling in Matching Markets. NBER Working Paper No. w16185. July 2010.
- Association of Professors of Gynecology and Obstetrics (APGO). Right Resident, Right Program, Ready Day One: Applicant Resources, 2025–2026 Cycle. Available at apgo.org/page/rrrapplicant.
- Council of Residency Directors in Emergency Medicine (CORD). EM Program Signaling Guidance for 2025–2026. Application Process Improvement Committee.
Next Step
Make every signal count.
A signal sent to a program where you are structurally screened out is a signal that never gets read. A residency match consultation aligns your program signaling strategy — both tiers — with the structural filters that programs apply first.
Schedule a Residency Match ConsultationIMGPrep is not associated with the NRMP®, the MATCH®, the ACGME, the AAMC, or the ECFMG®. Reproduction of NRMP figures requires written permission of the NRMP.
About Us
Established in 2005, IMGPrep assists International Medical Graduates in searching for U.S residency positions. We offer a complete set of affordable services. Our experts evaluate each IMG candidate and suggest what is needed for a medical residency match in the USA.
