How IMGs MATCH Into Psychiatry Residency: Screening, Holistic Review, and Selection Explained
March 19, 2026
2,516
PGY-1 psychiatry positions
offered · 2026 Match
offered · 2026 Match
97.4%
fill rate · 2,451 filled,
65 unfilled
65 unfilled
399
IMG matches · 177 U.S.
/ 222 non-U.S.
/ 222 non-U.S.
16.3%
IMG share of
filled positions
filled positions
Psychiatry is often called “IMG-friendly” — a label that leads many applicants to assume the match is relatively straightforward. In reality, the IMG Match Psychiatry process is selective and structured. Match outcomes are not determined by any single metric, but by how an application moves through each stage of the selection process. Understanding how that selection actually operates is the difference between matching and being filtered out.
For international medical graduates, the question is not simply whether psychiatry is IMG-friendly, but how IMGs successfully match into psychiatry — and why many do not. The IMG Match Psychiatry pathway rewards strategic alignment, not volume of applications. In 2024, U.S. citizen IMGs had a match rate of 67.0% and non-U.S. citizen IMGs 58.5%, compared with 93.5% for U.S. MD seniors. NRMP Charting Outcomes data shows Step 2 CK scores among matched applicants continuing to rise, reflecting an increasing academic baseline rather than a fixed cutoff. Psychiatry receives a large volume of IMG applicants, but it does not select broadly. Outcomes are determined by selective advancement, not broad acceptance.
Programs evaluate whether an application demonstrates both the capacity and the suitability to develop as a psychiatrist. That evaluation happens in three sequential stages, each asking a different question and applying a different filter. A single break at any stage removes the applicant — regardless of strength elsewhere. This is why two applicants with comparable scores can experience opposite outcomes.
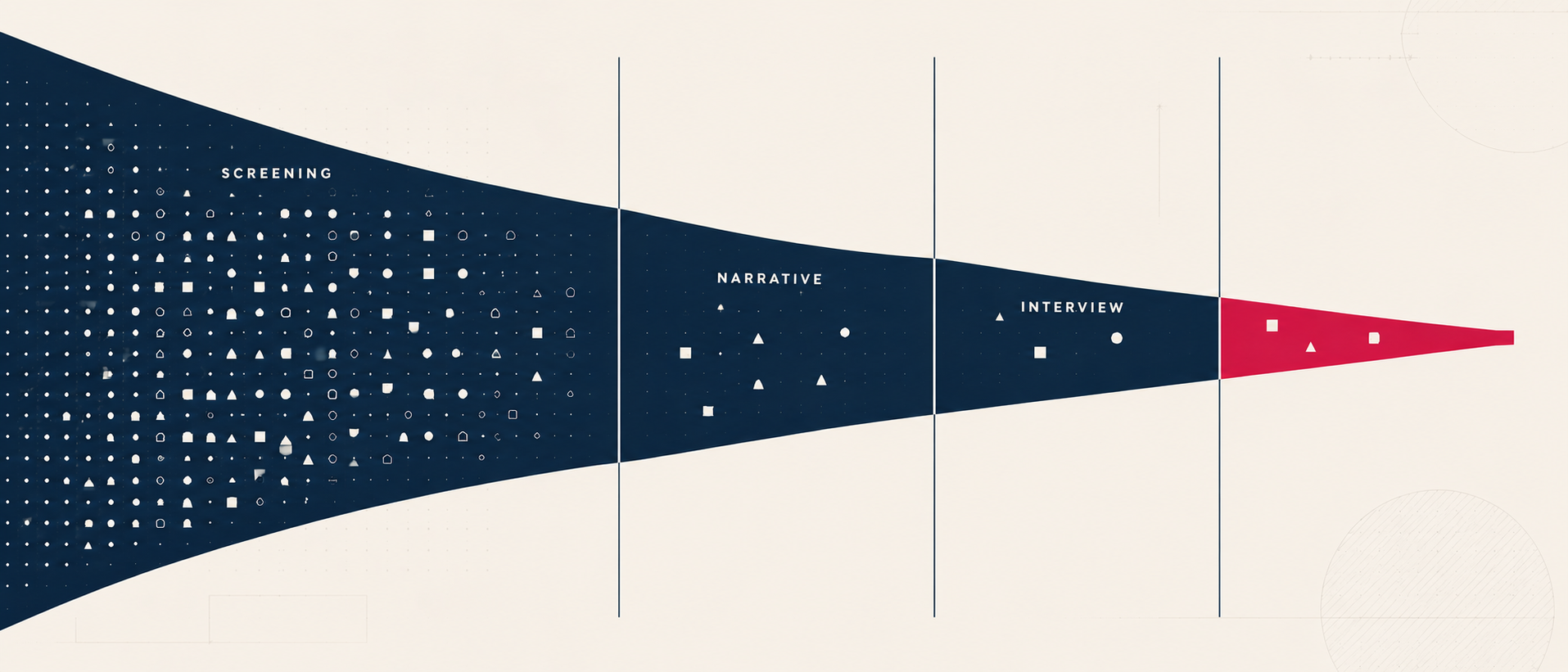
How the IMG Match Psychiatry Process Selects
Three sequential gates, each asking a different question and producing a smaller surviving pool.
Stage 1 · Screening
Who gets read
- USMLE Step 2 CK threshold
- Year of graduation
- Visa sponsorship status
- U.S. clinical experience
- ECFMG certification
Stage 2 · Narrative
Who advances
- Personal statement (applicant voice)
- Letters (external voice)
- MSPE (institutional voice)
- Experiences (behavioral evidence)
- Psychiatry-specific coherence
Stage 3 · Interview
Who is ranked
- Verbal communication
- Affective presence
- Listening & reflection
- Relational dynamics
- Narrative-behavior alignment
Stage 1 of the IMG Match Psychiatry Process — The Screening Filter
The majority of outcomes in the IMG Match Psychiatry process are determined before holistic review ever occurs. For many applicants, the application is never meaningfully read — not because it lacks potential, but because it does not pass initial screening thresholds. The imbalance between applicants and available positions is what drives screening intensity:
53,373
applicants registered for the 2026 Match
44,344
total positions offered nationally
2,516
of those in psychiatry
At this stage, programs are not evaluating fit. They are answering an operational question: does this application meet a baseline level that justifies further review? This is a problem of volume management under uncertainty, not final selection. At the program level it translates into large application volumes relative to a small number of interview spots, with only a fraction of applications reviewed in depth. The purpose of screening is not to identify the best applicants — it is to identify which applications can be reliably and efficiently advanced.
The signals screening relies on
Four variables function as high-efficiency filters, allowing programs to rapidly determine which applications can be advanced: Step 2 CK, year of graduation, visa status, and U.S. clinical experience. These signals are not used to fully understand the applicant. They determine whether the application meets a baseline level of interpretability and operational feasibility. This is the structural foundation of the SUVY framework.
Direct Answer
Following the transition of USMLE Step 1 to pass/fail scoring, over 83% of program directors reported placing greater emphasis on Step 2 CK. For IMGs — who historically relied on Step 1 to demonstrate academic mastery on the same scale as U.S. applicants — that differentiating signal is gone. Step 2 CK now functions as the dominant academic reliability signal.
Each program develops an internal comfort range, not always stated, but consistently applied:
| Score band | Screening interpretation |
|---|---|
| Lower | Concern about board passage or academic progression risk |
| Acceptable | Sufficient academic stability — application moves forward for further review |
| Higher | Expanded program access |
Score differences matter here. A 235 and a 260 are not equivalent: the higher score expands the number of programs that will review the application; the lower score may limit access at more selective programs. But it is not a ranking tool at this stage — it is a screening signal with downstream interpretive impact.
Passing screening does not mean an application is strong or competitive. It does mean the application demonstrates sufficient quantitative and structural signals to support further qualitative evaluation. Once past screening, the question — does this meet baseline criteria? — gives way to the holistic question: does this application make sense for psychiatry? This is the distinction between selective screening and holistic review.
Stage 2 of the IMG Match Psychiatry Process — Narrative Coherence and Goodness of Fit
Once an application clears screening, the program asks a different question: does this application demonstrate a credible goodness of fit for psychiatry? Does it portray a candidate whose academic, quantitative, and qualitative characteristics collectively indicate not only the potential to become a psychiatrist, but the potential to become a good one? Goodness of fit includes suitability for the specialty, commitment to the field, interpersonal and behavioral capacity, and the ability to fully engage with and benefit from training. Programs are not evaluating what the applicant did. They are evaluating what the application implies about who the applicant is becoming.
The four voices, and whether they agree
Four components carry the narrative, each speaking in a distinct voice. The decisive question is whether all of them signal the same underlying story.
Applicant voice
Personal Statement
External voice
Letters of Recommendation
Institutional voice
MSPE
Behavioral evidence
Experiences
A coherent application shows a personal statement reflecting specific, experience-based motivation; letters describing observable interpersonal and behavioral traits; an MSPE supporting professional reliability and growth; and experiences showing genuine progression toward psychiatry. The interpretation is a predictable trajectory. An incoherent application shows signals that do not align, a fragmented narrative, and an unclear trajectory — it does not form a stable or interpretable identity.
Where IMGs lose probability at this stage
| Failure pattern | What it looks like |
|---|---|
| No psychiatry-specific narrative | Broad or mixed specialty trajectory; psychiatry appears incidental rather than intentional |
| Single-voice narrative | The statement claims interest, but letters and experiences do not reinforce it; not externally validated |
| No behavioral evidence | Knowledge present, but no interpersonal signal and insufficient evidence of suitability |
Applicants are not filtered at this stage because they are weak. They are filtered because they are not interpretable as psychiatry-specific.
Passing Stage 2 means presenting a coherent, multi-source narrative that reduces uncertainty about trajectory, suitability, and capacity for development. What remains is the question the interview is built to answer: does this person actually function the way their application suggests?
Narrative & document strategy
The coherence programs read for is built deliberately, before applications open — personal statement, letters, MSPE, and experiences aligned to a single psychiatry-specific story. IMGPrep develops that narrative end-to-end.
Stage 3 of the IMG Match Psychiatry Process — The Interview
The interview is the convergence point. Screening established interpretability; the narrative built a working model; the interview is where that model is confirmed or breaks. The program is asking whether the person demonstrates the characteristics the application suggested — is the goodness of fit inferred on paper confirmed in real interaction?
Five signals are read in the room: verbal communication (clarity, nuance, flexibility), affective presence (warmth, engagement, emotional range), listening behavior (whether the applicant responds or merely answers), reflective thinking (real-time processing), and relational dynamics (interaction with faculty, residents, and coordinators). When these align with the narrative, behavioral signals confirm goodness of fit and the applicant is trusted. When they do not — inconsistent engagement, scripted responses, limited reflection, affect mismatch — the behavior fails to support the narrative.
Interview failure patterns
| Pattern | Signal to the program |
|---|---|
| Performative communication | Over-rehearsed, no spontaneity, flat affect — scripted, not relational |
| Low reflective depth | Describes events without insight — experience present, not processed |
| Interpersonal incongruence | Low engagement, affect mismatch — unclear relational capacity |
| Overly biomedical framing | Diagnosis-focused, no patient narrative — misaligned with psychiatry |
Passing does not mean a flawless performance — scripted excellence signals inauthenticity. It means real-time behavior confirms the goodness of fit inferred from the application. In the IMG Match Psychiatry process, the interview is where the strongest applications are confirmed. This is why interview preparation matters: the applicants ranked highly show narrative-behavior alignment, emotional fluency, reflective depth, and adaptive communication. At the ranking table, the question is no longer whether the applicant is qualified. It is: who do we trust most in our clinical and training environment?
Why Similar IMGs Have Different Outcomes
Two applicants with comparable scores routinely experience opposite outcomes. The difference is rarely a single metric. It is whether the application produces a coherent, interpretable signal at every gate. A single break — strong metrics with an incoherent narrative, a compelling statement unsupported by letters, or paper coherence the interview does not confirm — removes the applicant from contention, regardless of strength elsewhere.
A Stage-Aware IMG Match Psychiatry Strategy
1
Clear the screen
Target a Step 2 CK that expands program access; confirm ECFMG, visa, and year-of-graduation status early so the application is never filtered before it is read.
2
Build one coherent narrative
Align personal statement, letters, MSPE, and experiences to a single psychiatry-specific story so all four voices signal the same trajectory.
3
Confirm it in person
Prepare so real-time behavior reinforces the narrative — reflective, relational, psychiatry-oriented — rather than contradicting it.
4
Target where you are competitive
Apply to programs with a documented record of matching IMGs and where the SUVY profile is realistically competitive — not the full field.
Psychiatry Residency Strategy
Build a psychiatry application that holds at every stage.
IMGPrep structures the IMG Match Psychiatry application end-to-end — Step 2 CK positioning, U.S. clinical experience, narrative coherence across every document, and interview preparation. Customized program lists identify the psychiatry programs that have actually matched IMGs in recent cycles.
Related Reading on imgprep.com
→ IMG Friendly Psychiatry Programs: 2026 NRMP Data and State Distribution
→ IMG Friendly Programs and the SUVY Framework
→ Standardized Screening vs. Holistic Review in Residency Selection
→ MSPE for IMGs: A Strategic Guide
→ USMLE Changes 2026: Step 1, Step 2 CK, and Step 3 Update
→ 2026 U.S. IMG vs Non-U.S. IMG Residency Match Guide
→ Five-Year Analysis: IMG Residency Match Statistics, 2022–2026
→ Residency Personal Statement: Writing Tips and Red Flags
→ IMG Friendly Programs and the SUVY Framework
→ Standardized Screening vs. Holistic Review in Residency Selection
→ MSPE for IMGs: A Strategic Guide
→ USMLE Changes 2026: Step 1, Step 2 CK, and Step 3 Update
→ 2026 U.S. IMG vs Non-U.S. IMG Residency Match Guide
→ Five-Year Analysis: IMG Residency Match Statistics, 2022–2026
→ Residency Personal Statement: Writing Tips and Red Flags
Sources
- National Resident Matching Program. Results and Data: 2026 Main Residency Match. NRMP, May 2026. Psychiatry: 2,516 positions offered, 2,451 filled, 97.4% fill rate.
- National Resident Matching Program. Main Residency Match Results by State, Specialty, and Applicant Type, 2026. NRMP, 2026. Psychiatry IMG matches: 177 U.S. IMG, 222 non-U.S. IMG.
- National Resident Matching Program. Results and Data: 2024 Main Residency Match. NRMP, June 2024. U.S. IMG match rate 67.0%; non-U.S. IMG 58.5%; U.S. MD senior 93.5%.
- Wang A, et al. Effect of the USMLE Step 1 Pass/Fail Scoring System on the Residency Application Process. JAMA Netw Open. 2021;4(10):e2129557. 83.4% of program directors reported increased emphasis on Step 2 CK.
- National Resident Matching Program. Charting Outcomes: Program Director Survey Results, 2024 Main Residency Match. NRMP, August 2024.
IMGPrep is not associated with the NRMP®, the MATCH®, the ECFMG®, or the AAMC. Reproduction of NRMP figures requires written permission of the NRMP.
Contact Us
IMGPrep LLC, 4000 Legato Rd. Suite 1100
Fairfax, VA 22033
Fairfax, VA 22033
Fax: +1 (202) 751-2590
