Why Emergency Medicine Moved from ERAS to ResidencyCAS: Platform Alignment with Specialty-Specific Selection
April 18, 2026
IMGPrep Outcome Data
100% Match Rate
IMGPrep has maintained a 100% match rate for its Emergency Medicine IMG candidates over the past ten years within a highly selected cohort, reflecting a structured advisory process focused on specialty alignment, clinical preparation, and program-level targeting.
Introduction
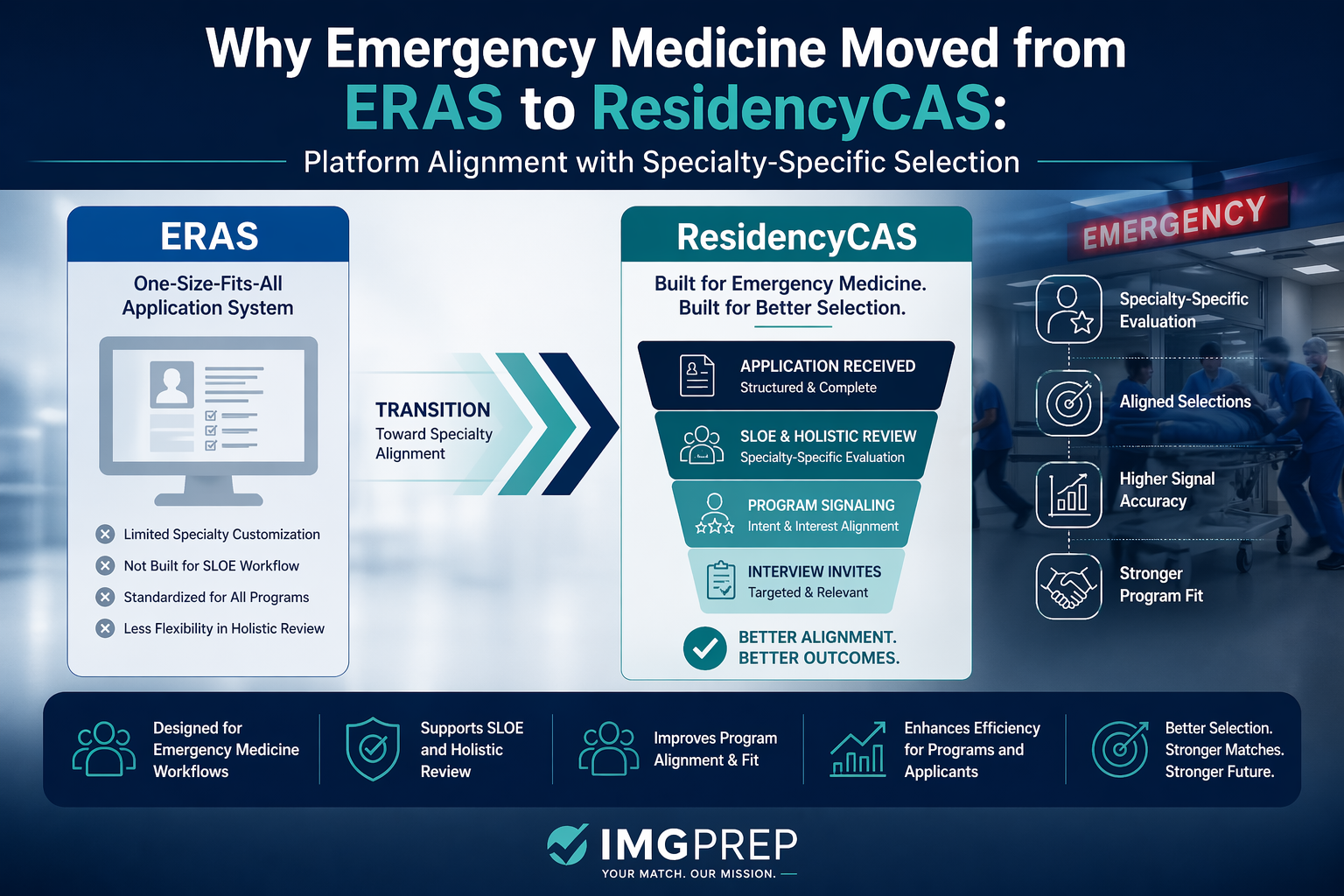
The Emergency Medicine ResidencyCAS transition, launched for the 2025–2026 application cycle, is the specialty’s structural response to a breakdown in applicant–program alignment observed during the 2022 and 2023 Match cycles. Emergency Medicine moved from ERAS to ResidencyCAS not to replace the platform, but to align application infrastructure with how the specialty actually evaluates applicants. In 2023, more than 550 positions remained unfilled despite an adequate applicant pool, indicating that the limitation was not supply, but the ability to identify and evaluate candidates who demonstrated specialty-specific alignment.
At the program level, this misalignment occurs within a constrained evaluation environment. Emergency Medicine programs receive approximately 700–750 applications per cycle, yet extend interviews to fewer than 200 applicants, with roughly 27% of applications excluded during initial screening.1 This compression creates a screening-dependent selection model in which early signal clarity determines access to interview and progression through the Match.
ResidencyCAS was developed to address this constraint by aligning the application infrastructure with how Emergency Medicine programs actually evaluate candidates.
The Structural Diagnosis Behind the Emergency Medicine ResidencyCAS Transition
The response from Emergency Medicine program leadership focused not on applicant quality, but on the structural environment in which applications were being reviewed. The 2022 cycle is instructive: programs received 3,081 applicants for 2,921 positions—a numerical surplus of applicants—yet 219 positions remained unfilled.2 The shortfall could not be explained by applicant volume alone. In 2023, even after applicant numbers declined below position counts, alignment failure accounted for the majority of the 554 unfilled positions.3 The application infrastructure was not successfully pairing available applicants with available positions—a breakdown the Emergency Medicine ResidencyCAS transition was designed to address.
The Electronic Residency Application Service (ERAS) had, for decades, functioned as the shared application platform across most specialties. Its architecture was designed to serve a broad set of programs by standardizing how applicants submit materials and how programs receive them. This generalist design produced substantial efficiency gains across graduate medical education, but it imposed uniform logic on specialties with fundamentally different selection mechanisms.
For Emergency Medicine, the misalignment was specific. The specialty does not primarily evaluate applicants through static document review. Emergency Medicine programs evaluate applicants through comparative, interaction-based, specialty-specific assessment—most prominently the Standardized Letter of Evaluation (SLOE), developed by the Council of Emergency Medicine Residency Directors to provide structured clinical appraisal across institutions.4 Program directors consistently identify the SLOE as the single most influential component of an application, ranked above USMLE scores, clinical grades, and any other individual element.4 ERAS was not designed to structure applications around this evaluation logic, and as application volumes continued to rise, the gap between how programs evaluated applicants and how ERAS organized those applications became an increasingly consequential operational constraint.
ResidencyCAS as the Specialty’s Structural Response
On October 8, 2024, the Council of Residency Directors in Emergency Medicine (CORD) announced a partnership with Liaison International to develop a dedicated application platform within the ResidencyCAS system.5 By the 2025–2026 cycle, 100% of Emergency Medicine programs had transitioned from ERAS to ResidencyCAS, making Emergency Medicine the second specialty—after Obstetrics and Gynecology—to operate on specialty-owned infrastructure.6
The stated objectives of the transition reflect a deliberate effort to address the alignment problem diagnosed after the 2022 and 2023 cycles: to improve how specialty-specific signals are communicated, to reduce financial barriers for applicants, to support holistic review through more contextualized application data, and to return ownership of specialty-wide application analytics to the specialty itself.57 The platform introduces structured fields—a uniform personal statement, Geographic Connections, defined experience categories—that convert applicant narratives into comparable signals programs can use within their evaluation frameworks.
ResidencyCAS is therefore best understood not as a replacement for ERAS, but as an alignment of the application infrastructure with how Emergency Medicine actually selects residents. For applicants, the implication of this framing is more important than any single feature of the new platform. The specialty has reorganized its application infrastructure around the evaluation logic it actually uses. Applicants who understand that logic can prepare accordingly. Applicants who do not will encounter a platform that is less forgiving of generic presentation than the system it replaced.
Example: Experience Interpretation Under Emergency Medicine ResidencyCAS
The contrast between ERAS and ResidencyCAS becomes concrete in how the same experience is framed for program review.
Weak — Non-Differentiated
Emergency Medicine Rotation. Participated in patient care, assisted with procedures, and worked with the clinical team.
Strong — ResidencyCAS-Aligned
Emergency Medicine Clinical Experience. Evaluated undifferentiated patients in a high-acuity setting, prioritizing triage and disposition under time constraints. Demonstrated clinical reasoning in initial assessment and contributed to team-based decision-making. This experience reflects readiness for Emergency Medicine’s pace, diagnostic breadth, and collaborative care model.
Interpretation: The distinction is not in the experience itself, but in how it is framed. ResidencyCAS converts experiences into evaluative signals. Programs are not assessing participation; they are assessing functional readiness within the specialty.
Common Emergency Medicine ResidencyCAS Application Errors
- Listing clinical experiences without demonstrating clinical reasoning or decision-making
- Reusing generalized narratives not adapted to structured prompts
- Overemphasizing participation rather than responsibility and progression
- Failing to use Geographic Connections strategically to signal regional alignment
- Treating experiences as a comprehensive list rather than a curated signal set
What Emergency Medicine ResidencyCAS Does Not Change
ResidencyCAS does not change the Match. The NRMP algorithm and final pairing process remain unchanged. What it changes is access—who is reviewed, who is interviewed, and how alignment is interpreted.
Applying to Emergency Medicine this cycle?
Submitting through ResidencyCAS is less forgiving of generic presentation than ERAS was. IMGPrep’s Residency Match Document Services structure your application materials around the specialty-specific signals Emergency Medicine programs actually evaluate.
Strategic Implications of Emergency Medicine ResidencyCAS for IMGs
For international medical graduates, the practical meaning of the transition follows directly from the structural analysis above.
Within the Emergency Medicine ResidencyCAS framework, program directors recommend that international medical graduates obtain at least two SLOEs, with timing structured to optimize evaluation visibility.8 An initial rotation early in the application cycle (May–June) allows for timely SLOE submission, while a second rotation (July–August) provides confirmatory evaluation. A third SLOE adds value only when it contributes additional signal—such as higher-acuity exposure or stronger comparative assessment—rather than duplicating prior evaluations.
Programs do not interpret SLOEs in isolation; they assess trajectory. Demonstrated improvement across rotations is often more informative than a single high-performing evaluation, as it reflects adaptability and integration into the specialty’s clinical environment.
Targeted application strategy becomes more decisive, not less. ResidencyCAS increases the precision with which programs assess alignment. Applications that clearly convey regional interest, specialty commitment, and readiness are interpreted more accurately; those that do not are filtered more efficiently. In a high-volume, low-signal environment, structured signals are recognized, while undifferentiated volume is not.
Program Targeting Framework
Emergency Medicine program accessibility for international medical graduates can be broadly understood across two screening dimensions.
| Flexible Graduation Cutoff | Strict Graduation Cutoff | |
|---|---|---|
| Visa Sponsorship Available | Moderate-access programs | Selective-access programs |
| No Visa Sponsorship | Limited-access programs | Highly restricted programs |
The majority of IMG-viable programs cluster in the upper-left quadrant, where visa sponsorship and graduation flexibility intersect. Identifying programs within this segment remains foundational to constructing an effective application strategy. For a curated, profile-matched view of this segment, see IMG-Friendly Emergency Medicine Residency Programs.
Structural barriers familiar to international medical graduates remain unchanged. Visa requirements, graduation year thresholds, and examination attempt histories continue to function as primary screening variables. Identifying programs whose screening parameters align with an applicant’s profile remains foundational. ResidencyCAS does not remove these constraints; it sharpens how applications are evaluated against them.
Across IMGPrep advisory cohorts, the most consistent determinant of interview conversion has not been total application volume, but the presence of clearly interpretable specialty-specific signals—particularly SLOE strength and Emergency Medicine rotation performance. Applicants with comparable academic metrics demonstrate significantly different outcomes based on how effectively these signals are communicated within the application.
Conclusion
The Emergency Medicine ResidencyCAS transition is most accurately understood as the specialty’s structural response to a diagnosed breakdown in how applicants and programs were being paired. The 2022 and 2023 cycles demonstrated that an adequate applicant pool and an adequate number of positions are not sufficient conditions for a functioning Match. What was missing was an infrastructure capable of supporting the specialty-specific evaluation through which Emergency Medicine actually selects residents. ResidencyCAS is that infrastructure.
For applicants, the significance of the transition is not primarily operational. The significance lies in what the change confirms about how Emergency Medicine selects residents—and therefore in how applicants should prepare. Programs continue to prioritize specialty-specific clinical evaluation over credential accumulation. They continue to weight direct observation over documentation. They continue to select for demonstrated alignment with the discipline. The platform has changed; the underlying selection logic has not.
The work of preparing a competitive Emergency Medicine application remains concentrated upstream of the platform itself—during US Emergency Medicine rotations, in the generation of credible SLOEs, and through the development of a clear specialty commitment that programs can recognize under conditions that reward precision over volume. ResidencyCAS is the infrastructure through which that preparation is now communicated. The preparation itself is what continues to determine access, evaluation, and selection.
Consult with IMGPrep
Emergency Medicine residency in the United States requires strong clinical preparation, targeted rotations, and careful application strategy. The transition to ResidencyCAS has restructured how applications are submitted and reviewed, but the underlying selection logic—centered on specialty-specific evaluation—remains consistent.
IMGPrep provides individualized advising for international medical graduates pursuing Emergency Medicine residency training in the United States.
Consult with IMGPrep to develop a structured Emergency Medicine application strategy, including clinical rotations, SLOE planning, program selection, and ResidencyCAS application preparation. For applicants who need support structuring their application materials, see Residency Match Document Services. Understanding and developing the application must go hand in hand with applying to the right programs, which is addressed through Customized Residency Program Lists.
Work With IMGPrep on Your Emergency Medicine Application
Our advisors have maintained a 100% Emergency Medicine match rate across a decade of IMG cohorts. Get an individualized strategy built around SLOE planning, rotation timing, and ResidencyCAS-aligned application preparation.
More on Emergency Medicine for IMGs
References
- National Resident Matching Program. Results and Data: 2024 Main Residency Match and Program Director Survey. NRMP; 2024.
- National Resident Matching Program. Results and Data: 2022 Main Residency Match. NRMP; 2022.
- Preiksaitis C, Krzyzaniak S, Bowers K, et al. The 2022 and 2023 Emergency Medicine Residency Match: A Cautionary Tale. Cureus. 2023.
- Love JN, Ronan-Bentle SE, Lane DR, Hegarty CB. The Standardized Letter of Evaluation for Postgraduate Training: A Concept Whose Time Has Come? Academic Medicine. 2016.
- Council of Residency Directors in Emergency Medicine. Emergency Medicine Collaboration with ResidencyCAS. CORD; 2024.
- Emergency Medicine Residents’ Association. Transition to ResidencyCAS 2025. EMRA Medical Student Council; 2025.
- American Medical Association. How emergency medicine’s new application could affect your Match. AMA; 2025.
- Pelletier-Bui AE, Schrepel C, Smith L, et al. Advising Special Population Emergency Medicine Residency Applicants: A Survey of Emergency Medicine Advisors and Residency Program Leadership. BMC Medical Education. 2020.
Contact Us
IMGPrep LLC, 4000 Legato Rd. Suite 1100
Fairfax, VA 22033
Fairfax, VA 22033
Fax: +1 (202) 751-2590
