Indian American Students Pursuing Medical Education in India: An Evidence-Based Overview
Introduction
The traditional pathway to medical practice in the United States requires an undergraduate degree, successful completion of the Medical College Admission Test (MCAT), four years of medical school, and residency training—a process spanning at least 11 years. An increasing number of Indian American students are choosing an alternative route: pursuing an MBBS (Bachelor of Medicine, Bachelor of Surgery) degree in India immediately after high school. While this pathway offers distinct advantages, it also presents significant, evidence-based challenges that prospective students and families must carefully consider.
The Appeal of Medical Education in India
Shorter Training Duration
The MBBS program in India requires 5.5 years total, including a mandatory one-year internship.[1] This represents a substantial time savings compared to the traditional U.S. pathway of four years undergraduate education plus four years of medical school.
Cost Considerations
Medical education costs in India are significantly lower than in the United States, particularly at government-funded institutions. However, the rapid expansion of private medical schools—which now constitute 57% of India's approximately 270 medical schools—has introduced considerable variability in both cost and quality.[1] Private institutions often charge substantially higher fees than government colleges.
Cultural Connection
For Indian American students, studying medicine in India offers an opportunity to connect with their heritage and gain clinical exposure to diseases and health conditions prevalent in South Asia.
Evidence-Based Challenges
Quality and Variability in Medical Education
The Indian medical education system faces documented quality concerns. Medical education experts have identified several systemic issues, including weak governmental regulation, questionable admission practices at some institutions, curricula that may lack relevance to contemporary health needs, and inadequate clinical exposure during training.[2][3][4] The compulsory internship year, intended to strengthen clinical skills, is often used primarily for studying for postgraduate entrance examinations rather than developing practical competencies.[1][3]
Accreditation by the Medical Council of India emphasizes documentation of infrastructure rather than educational outcomes and does not include comprehensive self-study processes.[3] The quality of education varies substantially between institutions, with some private medical schools operating without adequate equipment, qualified faculty, or standardized records.[1]
The Reality of Returning to Practice in the U.S.
Indian American students who complete medical training in India face substantial barriers when attempting to enter the U.S. healthcare system. As international medical graduates (IMGs), they must navigate a complex credentialing process that includes:
It is important to note that Indian American graduates of medical schools in India are classified as U.S. citizen IMGs rather than non-U.S. citizen IMGs. This distinction is meaningful within the residency selection process. Historically, U.S. citizen IMGs demonstrate higher match rates than non-U.S. citizen IMGs and do not face visa sponsorship barriers. While this classification remains less favorable than U.S. MD or DO graduate status, it is comparatively advantageous within the broader IMG cohort.
- ECFMG Certification: Submission of medical credentials, English language proficiency assessment, and successful completion of USMLE Step 1 and Step 2 Clinical Knowledge examinations[5]
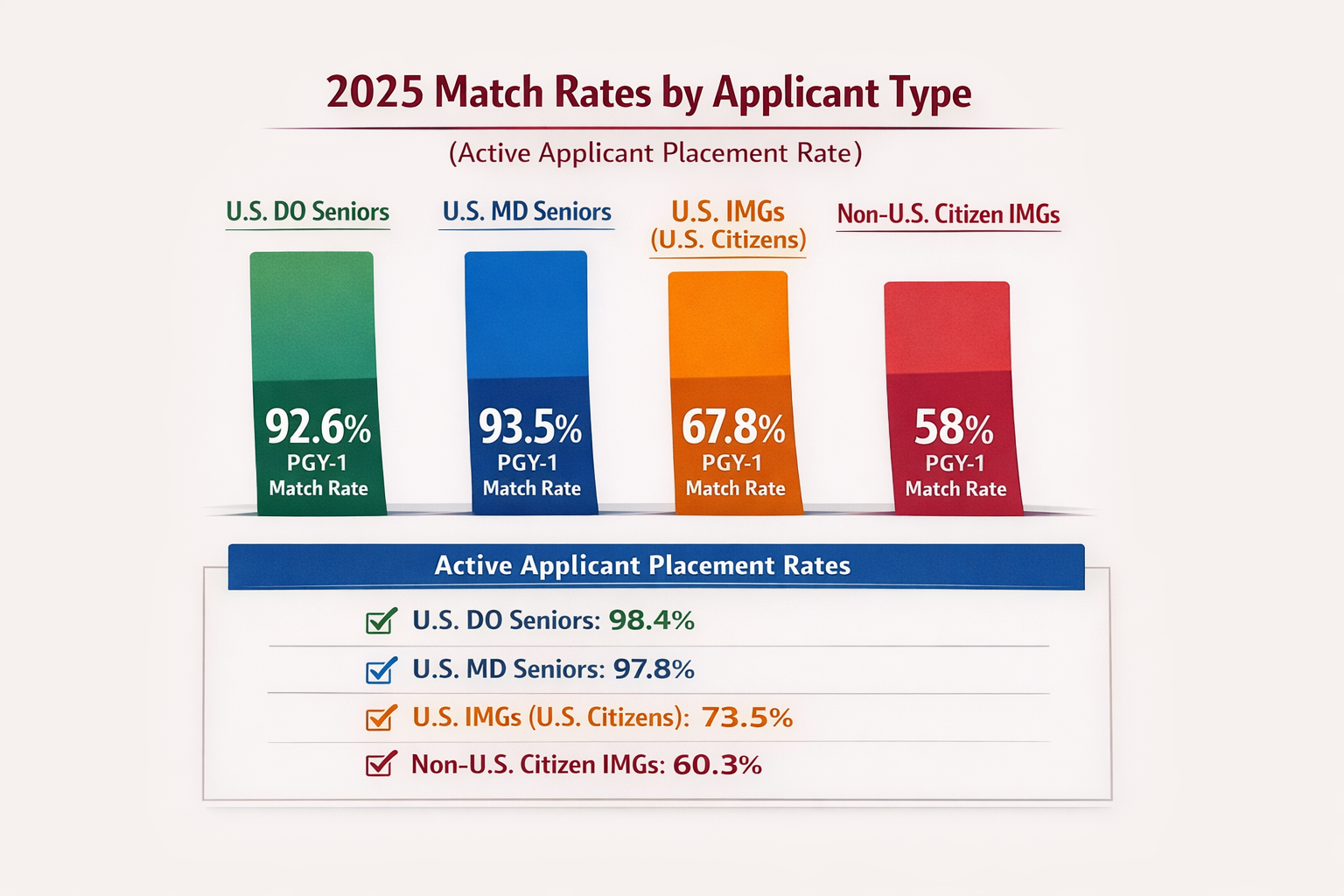
- Significantly Lower Match Rates: The 2025 match data reveal persistent disparities. U.S. MD seniors achieved a match rate of 93.5%, while U.S. citizen IMGs (including Indian American graduates) had a match rate of 67.8%—an improvement from 67.0% in 2024 but still 25.7 percentage points lower. Non-U.S. citizen IMGs matched at 58.0%. The following figure illustrates this persistent disparity over more than three decades:[5]
Figure 1
National Residency Matching Program Match Rates in the US
undefined
Despite the modest improvement in 2025, the gap between U.S.-trained physicians and IMGs has remained largely unchanged for decades. In 2025, non-U.S. citizen IMGs filled 6,653 positions (17.66% of total PGY-1 positions), representing a 13.45% year-over-year increase from 2024.[5]
- Impact of Pass/Fail Step 1: The conversion of USMLE Step 1 to pass/fail scoring has disproportionately disadvantaged IMGs, who previously relied on high numerical scores to demonstrate competence. In the 2022 match cycle (the last with numerical Step 1 scores), a U.S. MD senior with a Step 1 score of 235 (50th percentile) had a match rate above 98%, whereas the same score resulted in match rates of 82% for U.S. citizen IMGs and 63% for non-U.S. citizen IMGs. Remarkably, one in five non-U.S. citizen IMGs who achieved a score of 260 (95th percentile) went unmatched. The elimination of this objective metric has removed a key tool IMGs used to distinguish themselves.[5][6]
- Visa and Immigration Complexities: Non-U.S. citizen family members face lengthy immigration timelines, often resulting in extended family separation. The J-1 visa waiver program requires IMGs to return to their home countries for at least 2 years after training, with only 30 annual state waivers available for those committing to practice in high-need areas.[5][7][6]
- Limited Specialty Access: IMGs are significantly underrepresented in competitive specialties. While IMGs secured 23.5% of all residency positions in 2024, they filled only 10.4% of general surgery positions, 3.3% of dermatology positions, and 0.9% of orthopedic surgery positions.[5]
- Institutional Preferences: Research demonstrates that community-based programs are more likely to recruit IMGs than university programs. In 2017, 45% of community programs' interview positions were allocated to IMGs compared to only 15% at university programs. Factors influencing this disparity include departmental pressure, institutional priorities, and reputational concerns.[8]
Cultural and Professional Adaptation
IMGs face unique stressors beyond the match process. They must simultaneously navigate dual learning curves as immigrants and residents, adapt to different communication styles and professional behaviors, overcome biases and microaggressions, and often lack adequate mentorship and support networks.[9][10] Survey data from 7,817 IMG residents identified challenges navigating cultural differences (17%), the U.S. healthcare system (14%), distance from family (11%), and bureaucratic barriers (9%).[11]
Important Context: IMG Contributions and Outcomes
Despite these barriers, it is essential to recognize that IMGs constitute approximately 25% of the U.S. physician workforce and play a vital role in the healthcare system.[5][9] They disproportionately serve in primary care, fill positions in underserved rural and urban areas, and bring considerable clinical experience, research expertise, and diversity to medicine.[5][9][12]
Notably, research has demonstrated that patient outcomes for those treated by IMGs are comparable to or better than those treated by U.S. medical graduates. A large observational study of Medicare beneficiaries found that patients treated by international graduates had lower 30-day mortality rates than those treated by U.S. graduates (11.2% vs 11.6%).[5]
Making an Informed Decision
For Indian American students considering medical education in India, the decision requires careful evaluation of:
- Individual academic competitiveness: Recognition that even exceptional USMLE performance does not guarantee residency placement, and that the pass/fail Step 1 has removed a key differentiator
- Financial resources: Both for medical school and the extensive costs of USMLE examinations, ECFMG certification, residency applications, and potential multiple match attempts
- Specialty preferences: Understanding that competitive specialties may be largely inaccessible
- Family circumstances: Considering the impact of potential geographic separation and immigration complexities
- Institutional quality: Thoroughly researching specific medical schools, as quality varies dramatically across Indian institutions
Students from higher socioeconomic backgrounds and higher-income countries have demonstrated better match outcomes, suggesting that financial resources for test preparation, application processes, and multiple match attempts may influence success.[5]
Conclusion
The pathway of pursuing medical education in India and returning to practice in the United States is feasible but challenging. While the 2025 match data show modest improvement in IMG match rates (U.S. citizen IMGs increased from 67.0% to 67.8%), the evidence demonstrates substantial, persistent barriers to residency placement that have remained largely unchanged for decades. The gap between U.S. MD seniors (93.5%) and U.S. citizen IMGs (67.8%) remains 25.7 percentage points—a disparity that has persisted for over 30 years.
While many Indian American physicians have successfully navigated this route and made significant contributions to U.S. healthcare, prospective students must enter this pathway with realistic expectations, thorough preparation, and comprehensive understanding of the obstacles ahead. The recent conversion of USMLE Step 1 to pass/fail scoring has further complicated the landscape for IMGs, removing an objective metric that previously allowed high-performing international graduates to distinguish themselves.
The decision to pursue this pathway should be made only after careful consideration of the evidence-based challenges, consultation with physicians who have successfully completed this journey, and development of contingency plans should U.S. residency placement prove unsuccessful.
Consult IMGPrep
For families seeking a structured, data-driven evaluation of whether this pathway is appropriate, and for graduates navigating the return to United States residency training, consult with IMGPrep for individualized academic planning and evidence based residency match strategy.
International Medical School Selection ConsultationReferences
1. Human Resources for Health in India. Rao M, Rao KD, Kumar AK, Chatterjee M, Sundararaman T. Lancet (London, England). 2011;377(9765):587-98. doi:10.1016/S0140-6736(10)61888-0.
2. Relevance of the Flexner Report to Contemporary Medical Education in South Asia. Amin Z, Burdick WP, Supe A, Singh T. Academic Medicine : Journal of the Association of American Medical Colleges. 2010;85(2):333-9. doi:10.1097/ACM.0b013e3181c874cb.
3. Challenges and Issues in Medical Education in India. Supe A, Burdick WP. Academic Medicine : Journal of the Association of American Medical Colleges. 2006;81(12):1076-80. doi:10.1097/01.ACM.0000246699.94234.ab.
4. Medical Education in India: Current Challenges and the Way Forward. Solanki A, Kashyap S. Medical Teacher. 2014;36(12):1027-31. doi:10.3109/0142159X.2014.927574.
5. International Medical Graduates and the Physician Workforce. McElvaney OJ, McMahon GT. JAMA. 2024;332(6):490-496. doi:10.1001/jama.2024.7656.
6. Where Do International Medical Graduates Matriculate for Internal Medicine Training? A National Longitudinal Study. Reddy ST, Kisielewski M, Willett LL, et al. Journal of General Internal Medicine. 2021;36(8):2230-2236. doi:10.1007/s11606-020-06519-1.
7. International Medical Graduates: Promoting Equity and Belonging. Zaidi Z, Dewan M, Norcini J. Academic Medicine : Journal of the Association of American Medical Colleges. 2020;95(12S Addressing Harmful Bias and Eliminating Discrimination in Health Professions Learning Environments):S82-S87. doi:10.1097/ACM.0000000000003694.
8. Professional Challenges of non-U.S.-born International Medical Graduates and Recommendations for Support During Residency Training. Chen PG, Curry LA, Bernheim SM, et al. Academic Medicine : Journal of the Association of American Medical Colleges. 2011;86(11):1383-8. doi:10.1097/ACM.0b013e31823035e1.
9. International Medical Graduate Resident Wellness: Examining Qualitative Data From J-1 Visa Physician Recipients. Symes HA, Boulet J, Yaghmour NA, Wallowicz T, McKinley DW. Academic Medicine : Journal of the Association of American Medical Colleges. 2022;97(3):420-425. doi:10.1097/ACM.0000000000004406.
10. Easing the Entry of Qualified International Medical Graduates to U.S. Medical Practice. Andrews JS, Ryan AL, Elliott VS, Brotherton SE. Academic Medicine : Journal of the Association of American Medical Colleges. 2024;99(1):35-39. doi:10.1097/ACM.0000000000005310.
11. Quality of Care Delivered by General Internists in US Hospitals Who Graduated From Foreign Versus US Medical Schools: Observational Study. Tsugawa Y, Jena AB, Orav EJ, Jha AK. BMJ (Clinical Research Ed.). 2017;356:j273. doi:10.1136/bmj.j273.
12. Relationship Between Individual and Country-Level Socio-Economic Background, USMLE Step Scores, and Demographics of International Medical Graduates and Residency Match Results. Hunter DD, Campbell RL, Mullan AF, Anderson JR, Homme JL. BMC Medical Education. 2024;24(1):108. doi:10.1186/s12909-024-05052-7.
